ENDODONTICS AND ESTHETIC DENTISTRY(2)
Periodontal Probing
The depth of the sulcus and individual pockets are of concern to the treating dentist or endodontist. There are two main reasons for that concern. One is that if there is a combined periodontal endodontic problem associated with a tooth, the true cause of the problem is not only difficult to diagnose but could also be even more difficult to manage during treatment. The second issue is that if there is an isolated, narrow, but deep periodontal pocket somewhere around the tooth, a vertical root fracture has to be ruled out prior to any further restorative treatment. The pocket could be just a draining sinus tract from a necrotic and infected pulp. Endodontic therapy would then be indicated, and the pocket should heal without any periodontal therapy within days after the initial endodontic visit. The pocket could also be associated with a vertical root fracture, and if that is the case, the prognosis of the tooth is hopeless. Endodontic therapy would not clear up the pocket, nor would periodontal therapy. Extraction of the tooth or removal of the root would be the only treatment option.
Thermal Pulp Tests
In an effort to determine the vitality of a pulp, the cold test is probably the most commonly advocated. In the past, an "ice pencil" (water frozen in sterilized anesthetic cartridge and removed) (Figure 19-11) or an ice cube was the only consistent way to chill a tooth. But there are several problems with using frozen water: it is not very cold, so the stimulus may not be intense enough to penetrate through a porcelain crown, and cold water from the pencil could leak on adjacent teeth or gingival tissue, giving a false impression of pulpal vitality in the tooth that is being tested. However, in a tooth with an acute pulpitis, an ice pencil is an effective diagnostic tool. Recently, 1,1,1,2-tetrafluoroethane has become available in spray form (Endo-Ice, Hygenic,
Dry ice cylinders (Odontotest Thermal Pulp Tester, Miltex,
The response of a normal, healthy, vital pulp is sharp and quickly dissipates once the stimulus is removed. If the response is quicker, more intense, and prolonged, it usually indicates an irreversible pulpitis. When calcified pulp chambers or constricted canals exist, the response from an otherwise healthy tooth may be delayed or nonexistent. The reduced conductivity can mislead the operator. Therefore, other tests must be used to confirm negative responses.
When faced with teeth that are heavily restored, the final tests can be delayed until the tooth has been excavated, and the patient is in a provisional restoration. By wisely testing prior to final cementation, the true status of the pulp may be validated, and any changes that may have arisen during the fabrication interval can be appraised.
Heat is the least informative of the pulp tests and the most difficult to apply. Heated water applied to an individual tooth after it has been carefully isolated by a rubber dam is the most reliable method, but it is time consuming, and extreme care has to be taken so that there is no leaking under the rubber dam. It is recommended to start isolating and stimulating a tooth that is posterior to the one that is suspected to be heat sensitive and then move the rubber dam anteriorly tooth by tooth so that if there is a leak under the rubber dam, it will leak only on an already tested tooth. Heated temporary gutta-percha stopping applied to the lateral surface of a natural tooth or a metal surface of a veneer casting has been recommended, but it is difficult to control the heat, and the stopping has the tendency to stick on the tooth, causing prolonged stimuli. A rubber polishing wheel in a low-speed handpiece is an alternative also, but because it is difficult if not impossible to control the stimulus, this method is not recommended. The antiquated method of touching a tooth with a red hot burnisher should be avoided because of the risk of overheating the tooth and pulp, and there is no control over how intense the stimulus will be.
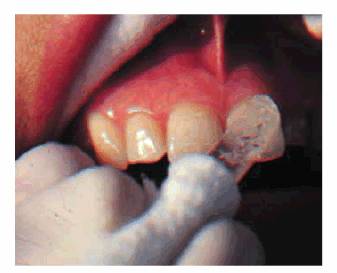
Figure 19-11: An ice pencil being applied to a maxillary central incisor tooth.
Figure 19-12: Endo-Ice (Hygenic) refrigerant.
TAGS:
0% (0)
0% (10)
Sponsored Links
Daliy Dental Topics
- on 01.11.2012 [endodontics]
- on 01.11.2012 [endodontics]
- on 01.11.2012 [endodontics]
- on 10.13.2011 [endodontics]
- on 12.15.2010 [endodontics]
- on 08.11.2010 [endodontics]
Useful Links
- Long Island College Hospital - [education]
- Faculty of Dental Medicine - H [education]
- The American Association of Or [organize]
- Summer Institute in Clinical D [organize]
- Academy of Osseointegration [organize]
- University of North Carolina a [education]
- American Orthodontic Society [article]
- American Equilibration Society [article]
- Niigata University - Japan [education]
- University of Buffalo [education]