ENDODONTICS AND ESTHETIC DENTISTRY(10)
Stressed Pulp
The dental literature is replete with methods and materials that demonstrate apparent success in preserving the integrity of the pulp, including the combination of sorghum molasses and English sparrow droppings.12 But as time passes, subtle changes take place in the pulp, creating an unhealthy and unreliable tissue to depend on as a sound foundation. This condition is often identified as "stressed pulp."
Abou-Rass considered the stressed pulp condition as an endodontic-restorative concept.1 He felt that it was of a clinical nature and not a histologic entity. It should be considered a preexisting pulpal possibility in every restored tooth prior to subjecting the tooth to further restorative procedures. If the pulp is stressed, its ability to react favorably to the new insult will be diminished.
For example, a mandibular molar, although repeatedly filled, has remained symptomless over a long period of time. A radiographic examination of the tooth demonstrates a deep occlusal amalgam and a large buccal composite restoration, recession of the pulp chamber, and narrowing of the root canals (Figure 19-36). Another example of stressed pulps is the maxillary incisors that underwent concussion injuries and two previous crown preparations. Although there were no pulp exposures and there were minimal symptoms, intentional extirpations were performed because it was felt that the pulps would not survive another restorative procedure (Figures 19-37A, 19-37B, and 19-37C). According to Abou-Rass's criteria, further insult to the affected (stressed) pulpal tissue would probably invite disaster. An intelligent decision would be elective endodontics, thereby intercepting potential problems.

Figure 19-36: Mandibular molar with a stressed pulp.

Figure 19-37A: View of maxillary central incisors following excavation of extensive caries. The pulps were not exposed.

Figure 19-37B: Radiograph of the same teeth. Note the minimal thickness of dentin adjacent to the pulp chambers.

Figure 19-37C: Root canal therapy completed on the maxillary central incisors.
Abou-Rass stated that the pulp's ability to recover from "stressed" pulp is relative to the type and duration of the injury, physiologic age, thickness of remaining dentin, and past trauma (impact injuries, repeated operative procedures). When all of these factors are examined and the patient's normal routine is changed because of vague symptoms, elective endodontic intervention must be considered. Another example of a stressed pulp is the patient with a maxillary anterior provisional restoration who required local anesthesia to remove the bridge 12 months after crown preparation and periodontal therapy because of pain in a maxillary central incisor tooth (Figures 19-38A, and 19-38B). The combined dental procedures have created stress on the pulpal complex that have exceeded the pulp's ability to repair. No patient wants to hear why it should have been done after the fact.

Figure 19-38A: Maxillary central incisor with a chronically inflamed (stressed) pulp.
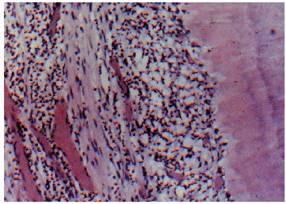
Figure 19-38B: A histologic section of chronic inflammation, irreversible pulpitis, with round cell infiltration. (Photograph courtesy of Dr. Harold R. Stanley.)
Elective Endodontics for Prosthetic Reasons
No tooth or components of a tooth should be sacrificed if the prognosis of the remaining dentition can be improved by its retention. Discussing elective endodontics vis-a-vis extensive restorations, Bohannan and Abrams felt that root canal therapy should he performed for reorientation of occlusal planes, reduction of crown:root ratios, and establishment of parallelism.7 A clinician faces many such situations when the overall esthetic and restorative results could be enhanced if the pulp was extirpated and the ideal root form was available. Unfortunately, the decision to perform the endodontics is often determined by issues other than what is beneficial to the patient (ie, economics, time, lack of skill or experience). Regardless, it is the duty of every diagnostician to evaluate and design each case with the goal of maximizing form, function, health, and esthetics. Therefore, when endodontic therapy enables the clinician to deliver the ideal restoration, why should the situation be compromised?
Endodontic Treatment Complications
An understanding of basic endodontic principles and a clearly defined restorative plan are essential prior to initiating root canal therapy. The final esthetic result should not be compromised by an inadequate approach. Therefore, various phases of endodontic treatment will be examined to see how they may enhance or preserve esthetics rather than detract from it. Although this may seem repetitious, the risk of performing endodontic procedures on restored teeth must be explained and accepted by the patient, and all discussions should be documented and recorded before a procedure is attempted.
- on 01.11.2012 [endodontics]
- on 01.11.2012 [endodontics]
- on 01.11.2012 [endodontics]
- on 10.13.2011 [endodontics]
- on 12.15.2010 [endodontics]
- on 08.11.2010 [endodontics]
- Long Island College Hospital - [education]
- Faculty of Dental Medicine - H [education]
- The American Association of Or [organize]
- Summer Institute in Clinical D [organize]
- Academy of Osseointegration [organize]
- University of North Carolina a [education]
- American Orthodontic Society [article]
- American Equilibration Society [article]
- Niigata University - Japan [education]
- University of Buffalo [education]